Lung nodules: size still matters
Anna Rita Larici,Alessandra Farchione,Paola Franchi,Mario Ciliberto,Giuseppe Cicchetti,Lucio Calandriello,Annemilia Del Ciello,Lorenzo Bonomo +7 more
TL;DR: Predictive models have been proposed as a potential means to overcome the limitations of a sized-based assessment of the malignancy risk for indeterminate pulmonary nodules.
read more
Abstract: The incidence of indeterminate pulmonary nodules has risen constantly over the past few years. Determination of lung nodule malignancy is pivotal, because the early diagnosis of lung cancer could lead to a definitive intervention. According to the current international guidelines, size and growth rate represent the main indicators to determine the nature of a pulmonary nodule. However, there are some limitations in evaluating and characterising nodules when only their dimensions are taken into account. There is no single method for measuring nodules, and intrinsic errors, which can determine variations in nodule measurement and in growth assessment, do exist when performing measurements either manually or with automated or semi-automated methods. When considering subsolid nodules the presence and size of a solid component is the major determinant of malignancy and nodule management, as reported in the latest guidelines. Nevertheless, other nodule morphological characteristics have been associated with an increased risk of malignancy. In addition, the clinical context should not be overlooked in determining the probability of malignancy. Predictive models have been proposed as a potential means to overcome the limitations of a sized-based assessment of the malignancy risk for indeterminate pulmonary nodules.
read more
Chat with Paper
AI Agents for this Paper
Find similar papers on Google Scholar, PubMed and Arxiv
Write a critical review of this paper
Analyze citations of this paper to find unaddressed research gaps
Figures
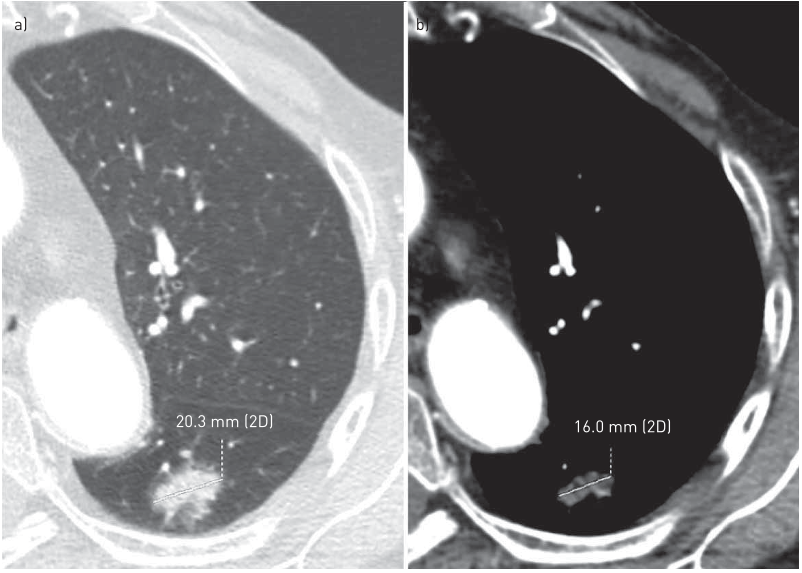
FIGURE 2 Disagreement in measuring the solid portion of a part-solid nodule when using different reconstruction algorithms and window settings. A part-solid nodule in the apical segment of left lower lobe is shown. a) By using a high-spatial frequency algorithm and the lung window, the measured maximum axial diameter of the solid portion of the nodule corresponds to 20.3 mm; b) by using a smooth algorithm and the mediastinal window, the measured maximum axial diameter of the solid portion of the nodule corresponds to 16 mm. 2D: two-dimensional. 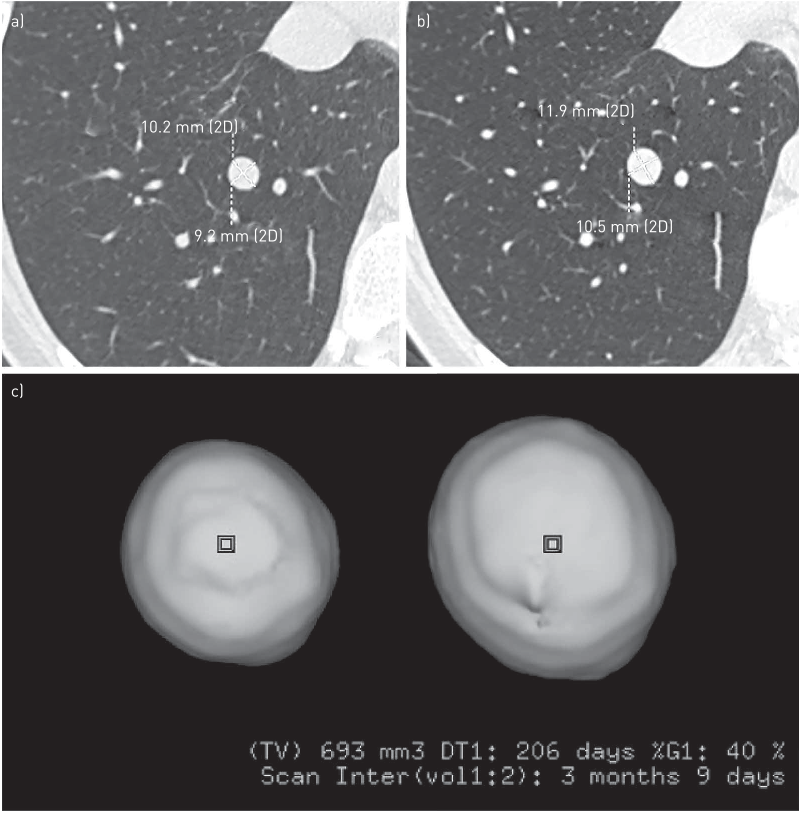
FIGURE 3 Volume evaluation during follow-up allows the detection of nodule growth over a shorter period of time compared to diameter estimation. a) Computed tomography (CT) axial image shows the same nodule located in the right lower lobe as reported in figure 1c; b) a 3-month follow-up axial CT image demonstrates minimal change in nodule diameters; c) conversely, nodule volume calculation using a three-dimensional (3D) volumetric method demonstrates a significant increase in volume within the range of malignancy. Histopathology revealed a carcinoid tumour. 2D: two-dimensional; TV: total volume; DT: volume doubling time; %G: volume increase; scan inter: scan interval. Squares in the nodule represent the starting points of the 3D analysis. 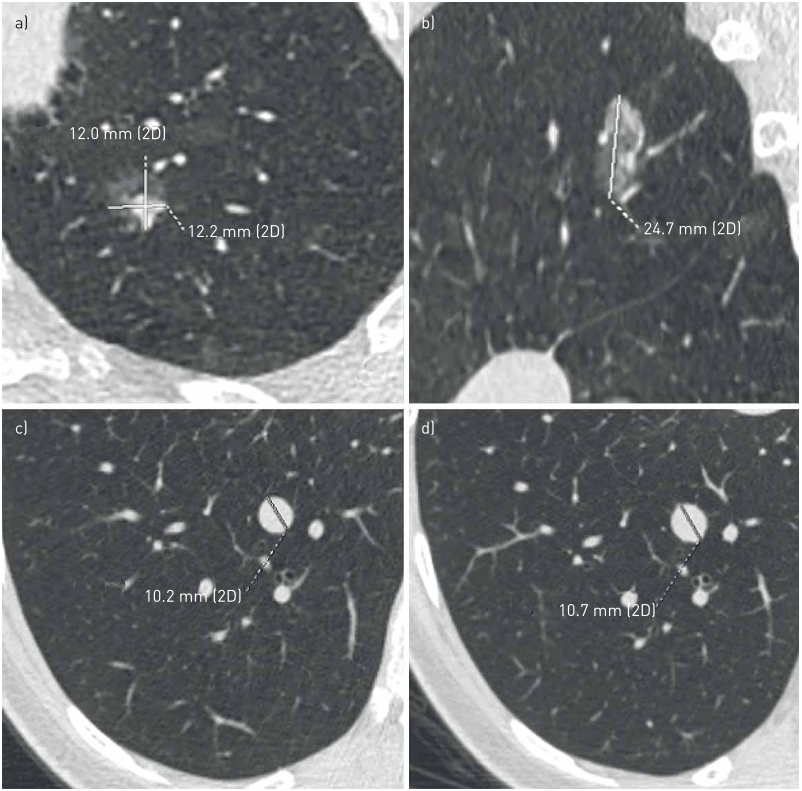
FIGURE 1 Limitations of two-dimensional (2D) measurements. The axial diameter may not be the maximum one in the evaluation of lung nodules. a) A small part-solid nodule in the apico-posterior segment of the left upper lobe, with a maximum axial diameter of 12×12.2 mm; b) the sagittal multiplanar reconstruction shows that the largest diameter of the same nodule is the sagittal one of 24.7 mm. The multiplanar evaluation of nodule diameter is especially important to document asymmetrical growth of nodules. c), d) The low level of agreement when measuring small nodules: for the same nodule in the right lower lobe two different diameter values have been reported by two readers. Considering the nearest whole diameter of the two values, it results in 1 mm difference in the maximum diameter, a significant difference when considering small nodules.



Citations
Radiomics Improves Cancer Screening and Early Detection
TL;DR: The inexorable improvements in radiomics to build more robust classifier models and the significant limitations to this development, including access to well-annotated databases, and biological descriptors of the imaged feature data are discussed.
Lung-RADS Version 1.1: Challenges and a Look Ahead, From the AJR Special Series on Radiology Reporting and Data Systems
Lydia Chelala,Rydhwana Hossain,Ella A. Kazerooni,Jared D. Christensen,Debra S. Dyer,Charles S. White +5 more
TL;DR: Lung-RADS as discussed by the authors provides a common lexicon and standardized nodule follow-up management paradigm for use when reporting lung cancer screening (LCS) low-dose CT (LDCT) chest examinations and serves as a quality assurance and outcome monitoring tool.
68
Diagnosis and management of peripheral lung nodule
TL;DR: A solitary pulmonary nodule (SPN) is a well-defined radiographic opacity up to 3 cm in diameter that is surrounded by unaltered aerated lung that is an incidental finding on chest radiographs and chest CT scans.
56
Application of Radiomics in Predicting the Malignancy of Pulmonary Nodules in Different Sizes.
TL;DR: The radiomic T1a model showed superior prediction performance to the T1b and T1c models, and the best performance in terms of AUC and sensitivity was found for predicting the malignancy of T1A PN.
52
References
Benefit of overlapping reconstruction for improving the quantitative assessment of CT lung nodule volume.
TL;DR: These results support the use of overlapping reconstruction to improve the quantitative assessment of nodule size with CT imaging.
Effect of varying CT section width on volumetric measurement of lung tumors and application of compensatory equations.
Helen T. Winer-Muram,S. Gregory Jennings,Cristopher A. Meyer,Yun Liang,Alex M. Aisen,Robert D. Tarver,Ronald C. McGarry +6 more
TL;DR: How volume measurements of simulated and clinical lung tumors at standard computed tomographic (CT) lung window and level settings vary with section width and to derive and apply compensatory equations is determined.
Noncalcified Lung Nodules: Volumetric Assessment with Thoracic CT
TL;DR: The review points to the need for continued research to examine volumetric accuracy as a function of a multitude of interrelated variables involved in the assessment of lung nodules.
Small pulmonary nodules: volume measurement at chest CT--phantom study.
Jane P. Ko,Henry Rusinek,Erika L. Jacobs,James S. Babb,Margrit Betke,Georgeann McGuinness,David P. Naidich +6 more
TL;DR: Three-dimensional methods for quantifying pulmonary nodule volume at computed tomography (CT) and the effect of imaging variables were studied by using a realistic phantom to show that a PVM is promising for volume quantification and follow-up of nodules.
The IASLC Lung Cancer Staging Project: Proposals for Coding T Categories for Subsolid Nodules and Assessment of Tumor Size in Part-Solid Tumors in the Forthcoming Eighth Edition of the TNM Classification of Lung Cancer
William D. Travis,Hisao Asamura,Alexander A. Bankier,Mary Beth Beasley,Frank C. Detterbeck,Douglas B. Flieder,Jin Mo Goo,Heber MacMahon,David P. Naidich,Andrew G. Nicholson,Charles A. Powell,Mathias Prokop,Ramón Rami-Porta,Valerie W. Rusch,Paul Van Schil,Yasushi Yatabe,Peter Goldstraw,David Ball,David G. Beer,Ricardo Beyruti,Vanessa Bolejack,Kari Chansky,John Crowley,Wilfried Eberhardt,John G. Edwards,Françoise Galateau-Salle,Dorothy Giroux,Fergus V. Gleeson,Patti A. Groome,James Huang,Catherine Kennedy,Jhingook Kim,Young Tae Kim,Laura Kingsbury,Haruhiko Kondo,Mark Krasnik,Kaoru Kubota,Antoon Lerut,Gustavo Lyons,Mirella Marino,Edith M. Marom,Jan P. van Meerbeeck,Alan Mitchell,Takashi Nakano,Anna K. Nowak,Michael D Peake,Thomas W. Rice,Kenneth E. Rosenzweig,Enrico Ruffini,Nagahiro Saijo,Jean-Paul Sculier,Lynn Shemanski,Kelly G. Stratton,Kenji Suzuki,Yuji Tachimori,Charles F. Thomas,William D. Travis,Ming-Sound Tsao,Andrew T. Turrisi,Johan Vansteenkiste,Hirokazu Watanabe,Yi-Long Wu,Paul Baas,Jeremy J. Erasmus,Seiki Hasegawa,Kouki Inai,Kemp H. Kernstine,Hedy L. Kindler,Lee M. Krug,Kristiaan Nackaerts,Harvey I. Pass,David C. Rice,Conrad Falkson,Pier Luigi Filosso,Giuseppe Giaccone,Kazuya Kondo,Marco Lucchi,Meinoshin Okumura,Eugene H. Blackstone +78 more
TL;DR: Codes for the primary tumor categories of AIS and minimally invasive adenocarcinoma (MIA) and a uniform way to measure tumor size in part‐solid tumors for the eighth edition of the tumor, node, and metastasis classification of lung cancer are proposed.
Related Papers (5)
Annette McWilliams,Martin C. Tammemägi,John R. Mayo,Heidi C. Roberts,Geoffrey Liu,Kam Soghrati,Kazuhiro Yasufuku,Simon Martel,Francis Laberge,Michel Gingras,S. Atkar-Khattra,Christine D. Berg,Kenneth R. Evans,Richard J. Finley,John Yee,John C. English,Paola Nasute,John R. Goffin,Serge Puksa,Lori Stewart,Scott Tsai,Michael R. Johnston,Daria Manos,Garth Nicholas,Glenwood D. Goss,Jean M. Seely,Kayvan Amjadi,Alain Tremblay,Paul Burrowes,Paul MacEachern,Rick Bhatia,Ming-Sound Tsao,Stephen Lam +32 more
Samuel G. Armato,Geoffrey McLennan,Luc Bidaut,Michael F. McNitt-Gray,Charles R. Meyer,Anthony P. Reeves,Binsheng Zhao,Denise R. Aberle,Claudia I. Henschke,Eric A. Hoffman,Ella A. Kazerooni,Heber MacMahon,Edwin J. R. van Beek,David F. Yankelevitz,Alberto Biancardi,Peyton H. Bland,Matthew S. Brown,Roger Engelmann,Gary E. Laderach,Daniel Max,Richard C. Pais,David Qing,Rachael Y. Roberts,Amanda R. Smith,Adam Starkey,Poonam Batra,Philip Caligiuri,Ali Farooqi,Gregory W. Gladish,C. Matilda Jude,Reginald F. Munden,Iva Petkovska,Leslie E. Quint,Lawrence H. Schwartz,Baskaran Sundaram,Lori E. Dodd,Charles Fenimore,David Gur,Nicholas Petrick,John Freymann,Justin Kirby,Brian Hughes,Alessi Vande Casteele,Sangeeta Gupte,Maha Sallam,Michael D. Heath,Michael Kuhn,Ekta Dharaiya,Richard Burns,David Fryd,Marcos Salganicoff,Vikram Anand,Uri Shreter,Stephen Vastagh,Barbara Y. Croft,Laurence P. Clarke +55 more